By
By
ProcellaRX Healthcare IT Series · Episode 01 · March 26, 2026
We billed this session as a tactical conversation about SaaS evidence fragmentation and defensible decision trails. What emerged instead was a diagnosis of something deeper — and if you missed it, this post is your briefing.
On March 26, I had the privilege of hosting five remarkable women at the intersection of healthcare strategy, clinical operations, digital health, patient advocacy, and global systems design. The original abstract promised a practical session on reconstructing IT decisions under pressure. The conversation we actually had showed why that capability problem is downstream of something more fundamental: a trust infrastructure problem.
This is the blog post that bridges those two conversations.
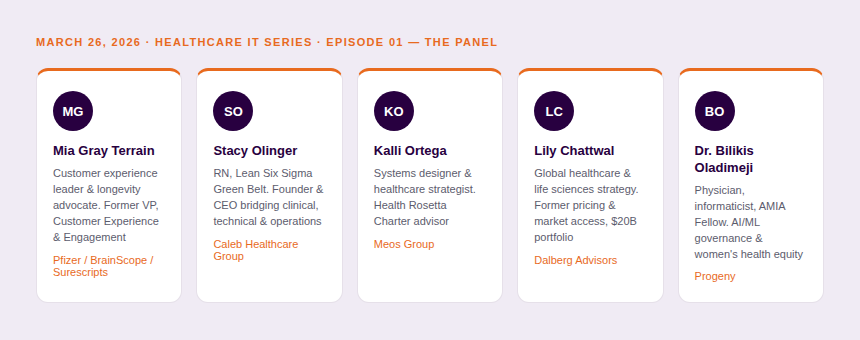
Meet the panel
Before we get into the substance, I want to properly introduce the women who made this conversation what it was.
The gap — and why it matters
The original abstract described a problem every Healthcare IT leader knows viscerally: when an audit, incident, or investigation hits, evidence is scattered across SaaS platforms, tickets, emails, and shared drives. The instinct is to build better logging, tighter workflows, cleaner audit trails. Good instincts. But not the root cause.
What this panel surfaced is that evidence fragmentation is a symptom. The disease is that we designed health systems — clinical workflows, data platforms, patient-facing tools, SaaS stacks — without making trust the load-bearing structure. When trust isn't designed in, defensibility becomes a retrofit. And retrofits are always expensive.
What trust actually means — and why the definition matters for IT
I opened by asking each panelist to define trust. What came back wasn't soft. It was a governance framework.
"It comes down to integrity, transparency, and accountability. Are you doing what you say you do? Are your decisions available for review by others? Are you holding yourself — and your ecosystem — accountable?" — Kalli Ortega, Founder & CEO, Meos Group
Integrity. Transparency. Accountability. For any Healthcare IT leader reading this: those are also the three pillars of a defensible decision record. Kalli wasn't describing compliance theater — she was describing the same architecture that makes an audit survivable.
Lily brought the data layer into focus, noting that trust in 2026 means asking: what's being captured, how is it stored, how is it shared, who owns the ultimate decisions, and how does it connect to financial data? For IT leaders managing SaaS stacks across a health system, this isn't abstract. It's your vendor contracts, your data governance policies, and your incident response protocols — all at once.
Mia grounded it in the patient experience:
"Trust is that a customer — a patient — believes you will deliver on your promise. It takes time to build. It takes very little to lose." — Mia Gray Terrain
And Stacy added what I think is the most operationally important dimension: trust is reciprocal. It extends in both directions. A trust bank is built. And it can be depleted. That framing should live in every healthcare organization's risk register.
When the system fails — a real example
I shared a story from my own life that I think crystallizes the entire problem we're here to solve. My partner Danielle, who is living with stage four prostate cancer, had her records systematically miscoded — wrong gender, wrong biological reference ranges applied to her blood work results. A cascade of human errors, each small, each plausible in isolation, compounding in a system that never surfaced the contradiction.
Here's what struck me: the system held more accurate data about her than the humans entering it. The data was there. The evidence existed. But because accountability for data quality was diffuse — spread across billing, clinical entry, EHR configuration, and a dozen SaaS touchpoints — no one owned the error, and no one caught it until it mattered.
This is your defensibility problem. Not theoretical. Lived.
Dr. Bilikis extended this into a systems design observation that every IT architect should hear: every actor in the care ecosystem — patient, clinician, billing specialist, coder, medication administrator — must have both the capacity and the clear role definition to play their part accurately. When the ecosystem doesn't define those roles and equip those actors, errors don't stay isolated. They compound. And when they compound, reconstructing what happened becomes nearly impossible.
The SaaS world made this harder — and now AI is amplifying the stakes
The original abstract called out SaaS fragmentation. The panel confirmed it from multiple vantage points. Lily noted that the data question now involves synthetic data — models trained on realistic fake health data that can be used to probe vulnerabilities in health systems. The threat surface for Healthcare IT isn't just breaches anymore; it's adversarial probing of the evidence architecture itself.

Stacy raised something that doesn't get enough airtime in technical discussions: when AI scribes and documentation tools enter clinical workflows, the margin of error in AI-generated summaries is real — and it varies dramatically across platforms. Her advice: always request the actual transcript, not just the summary. Because if you ever need to defend a clinical decision, the summary is not the evidence. The transcript is.
For IT leaders, that is an immediate architectural requirement. If your AI documentation tools don't preserve the source transcript alongside the generated summary, you are building a defensibility gap into your own stack.
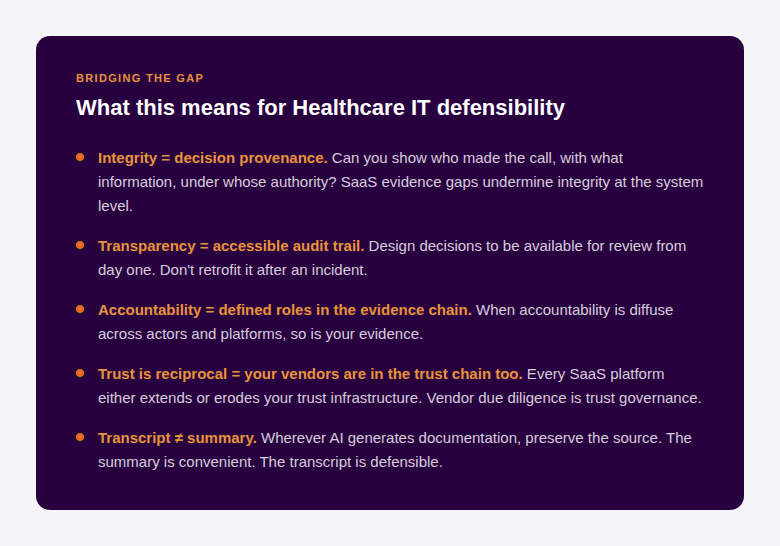
Bridging the gap: what this means for Healthcare IT defensibility
Here is how the panel's conversation translates directly into the original promise of this session:
The global lens: what leapfrogging teaches us about legacy debt
Lily had just returned from an AI summit in India, where she helped facilitate a workshop on reimagining primary care in markets like Bangladesh — countries with strong digital public infrastructure but without the legacy system debt of a U.S. health network. Her observation was quietly devastating for anyone managing a complex American health system:
Countries without legacy systems get to start with the problem statement. Countries with Epic and Cerner integrations start with the constraint set. If you're building defensibility into a 20-year-old SaaS stack layered over an aging EHR, you are fighting gravity. The question isn't whether to invest in trust infrastructure — it's whether you invest now or pay a steeper price during the next audit, incident, or investigation.
Final counsel from the panel
I asked each panelist for one piece of advice — to their networks, to IT directors, to anyone within their sphere of influence.
"For IT directors: your role is so important. Work closely with business and clinical owners from the beginning. It should never be a surprise when something isn't working. And bring the lens of stewardship — because AI is also creating real fraud and misuse, and you are the steward of trust in that environment." — Lily Chattwal, Dalberg Advisors
"The heart of medicine is connecting the healer with those who need to be healed. Technology should remove every barrier to that moment — not add new ones. The greatest tech in the world does not replace the human element of that relationship." — Stacy Olinger, Caleb Healthcare Group
"When you are the patient, you are the person who matters most in the equation. You have the power to advocate, to ask until you have real answers, and to vote with your feet if the care isn't right. Whatever systems we build need to give you that authority — not quietly take it away." — Dr. Bilikis Oladimeji, Progeny
Mia closed the loop: focus on the human with the problem, not the technology solving it. That will almost always also solve the business problem — but not the other way around.
Connect with Miya Gray Terrain; Stacy Olinger; Kalli Ortega; Lily Chattwal; Dr. Bilikis Oladimeji
I started my career believing that quality was a compliance function. I've spent two decades learning that quality — real quality — is a trust function. What these women articulated with precision and candor is that the defensibility problem Healthcare IT faces today isn't solvable with better logging software. It's solvable by designing systems where integrity, transparency, and accountability are the architecture — not the audit.
My consistent position: quality is not proprietary. These learnings belong to the field. Share them. Challenge the legacy thinking. And stop treating defensibility as something you build after the problem. Build it in.
This is the first webinar in our Healthcare IT series. Questions that didn't get answered live will be addressed in follow-up posts. If this conversation sparked something for you — whether you're an IT director, a clinical operations leader, a compliance officer, or a patient — I want to hear from you.
Dori Gonzalez-Acevedo is the Founder & CEO of ProcellaRX, a strategic life sciences consulting firm specializing in digital validation and quality transformation. Connect on LinkedIn · procellarx.co